
This post was originally published on Richard’s Blog.
The title of this post might refer to the very, very famous trials of Amanda Knox in the case of the murder of Meredith Kercher. However, I am writing about a case that is much less known outside of Italy (neither victim nor alleged murderer was a rich American girl). This is the case of Daniela Poggiali, a nurse suspected by the media and accused by prosecution experts of having killed around 90 patients in a two-year killing spree terminated by her arrest in April 2014. She has just been exonerated after a total of three years in prison with a life sentence as well some months of pre-trial detention. This case revolved around statistics of an increased death rate during the shifts of a colourful nurse. I was a scientific expert for the defence, working with an Italian colleague, Julia Mortera (Univ. Rome Tre), later assisted by her colleague Francesco Dotto.
Lucia de Berk
Piet Groeneboom and I worked together on the statistics of the case of Lucia de Berk, see our paper in Chance [Reference]. In fact, it was remarkable that the statistical community in the Netherlands got so involved in that case. A Fokke and Sukke cartoon entitled “Fokke and Sukke know it intuitively” had the exchange “The probability that almost all professors of statistics are in agreement … is obviously very small indeed”.
Indeed, it wasn’t. That was one of the high points of my career. Another was Lucia’s final acquittal in 2010, at which the judges took the trouble to say out loud, in public, that the nurses had fought heroically for the lives of their patients; lives squandered, they added, by their doctors’ medical errors.
At that point, I felt we had learnt how to fight miscarriages of justice like that, of which I rapidly became involved in several. So far, however, with rather depressing results. Till a couple of months ago. This story will not have much to do with mathematics. It will have to do with simple descriptive statistics, and I will also mention the phrases “p-value” and “Bayes’ rule” a few times. One of the skills of a professional statistician is the abstraction of messy real-world problems involving chance and data. It’s not for everybody. Many mathematical statisticians prefer to prove theorems, just like any other mathematician. In fact, I often do prefer to do that myself, but I like more being able to alternate between the two modes of activity, and I do like sticking my nose into other people’s business, and learning about what goes on in, for instance, law, medicine, or anything else. Each of the two activity modes is a nice therapy for the frustrations which inevitably come with the other.
Messy Excel spreadsheets
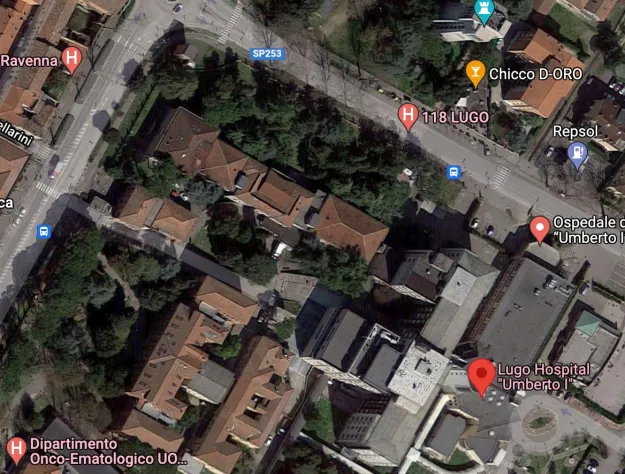
The Daniela Poggiali case began, for me, soon after the 8th of April, 2014, when it was first reported in international news media. A nurse at the Umberto I hospital in the small town of Lugo, not far from Ravenna, had been arrested and was being investigated for serial murder. She had had photos of herself taken laughing, close to the body of a deceased patient, and these “selfies” were soon plastered over the front pages of tabloid media. Pretty soon, they arrived in The Guardian and The New York Times. The newspapers sometimes suggested she had killed 93 patients, sometimes 31, sometimes it was other large numbers. It was suspected that she had used Potassium Chloride on some of those patients. An ideal murder weapon for a killer nurse since easily available in a hospital, easy to give to a patient who is already hooked up to an IV drip, kills rapidly (cardiac arrest – it is used in America for executions), and after a short time hard to detect. After death, it redistributes itself throughout the body where it becomes indistinguishable from a normal concentration of Potassium.

Many features of the case reminded me strongly of the case of Lucia de Berk in the Netherlands. In fact, it seemed very fishy indeed. I found the name of Daniela’s lawyer in the online Italian newspapers, Google found me an email address, and I sent a message offering support on the statistics of the case. I also got an Italian statistician colleague and good friend, Julia Mortera, interested. Daniela’s lawyer was grateful for our offer of help. The case largely hinged on a statistical analysis of the coincidence between deaths on a hospital ward and Daniela’s shifts there. We were emailed pdfs of scanned pages of a faxed report, written by a pathologist/toxicologist and an epidemiologist, of around 50 pages containing results of statistical analyses of times of shifts of all the nurses working on the ward, and times of admission and discharge (or death) of all patients, during much of the period 2012 – 2014. There were a further 50 pages (also scanned and faxed) of appendices containing print-outs of the raw data submitted by hospital administrators to police investigators. Two huge messy Excel spreadsheets.
Several deaths a week
Daniela Poggiali worked on a very large ward with very many very old patients, many suffering terminal illnesses. Ages ranged from 50 up to 105, mostly around ninety. The ward had about 60 beds and was usually quite fully occupied. Patients tended to stay one to two weeks in the hospital, admitted to the hospital for reasons of acute illness. There were on average several deaths every week; some days none, some days up to four. Most patients were discharged after several weeks in the hospital to go home or to a nursing home. It was an ordinary “medium care” nursing department (i.e., not an Intensive Care unit).
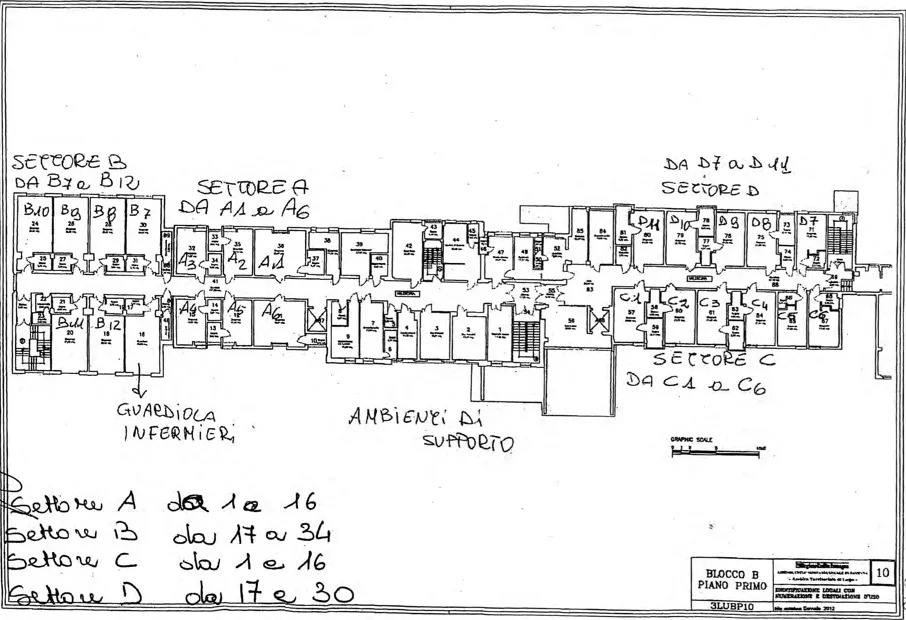
Some very simple statistics showed that the death rate on days when Poggiali worked was much higher than on days when she did not work. A more refined analysis compared the rate of deaths during the hours she worked with the rate of deaths during the hours she was not at work. Again, her presence “caused” a huge excess, statistically highly significant. A yet more refined analysis compared the rate of deaths while she was at work in the sectors where she was working with the rate in the opposite sectors. What does this mean? The ward was large and spread over two long wings of one floor of a large building, “Blocco B”, probably built in the sixties.

Between the two wings were central “supporting facilities” and also the main stairwell. Each wing consisted of many rooms (each room with several beds), with one long corridor through the whole building, see the floor plan below. Sector A and B rooms were in one wing, first A and then B as you you went down the corridor from the central part of the floor. Sector C and Sector D rooms were in the other wing, opposite to one another on each side of the corridor. Each nurse was usually detailed in her shifts to one sector, or occasionally to the two sectors in one wing. While working in one sector, a nurse could theoretically easily slip into a room in the adjacent sector. Anyway, the nurses often helped one another, so they often could be found in the “wrong sector”, but not often in the “wrong wing”.
The authors of the report went on to look at the death rates while Daniela was at work in different periods. They noticed that it was higher in 2013 than in 2012, even higher in the first quarter of 2014, then – after Daniela had been fired – it was much, much less. They conjectured that she was killing more and more patients as time went by, till the killing stopped dead on her suspension and arrest.
The prosecutor’s fallacy
The authors certainly knew that, in theory, other factors might be the cause of an increased death rate on Poggiali’s shifts. They were proud of their innovative approach of relating each death that occurred while Daniela was at work to whether it occurred in Daniela’s wing or in the other. They wrote that in this way they had controlled for confounders, taking each death to provide its own “control”. (Similarly, in the case of Lucia de B., statistician Henk Elffers had come up with an innovative approach. In principle, it was not a bad idea, though all it showed was that nurses are different). The authors did not control for any other confounding factors at all. In their explanation of their findings to the court, they repeatedly stated categorically that the association they had found must be causal, and Daniela’s presence was the cause. Add to this that their clumsy explanation of p-values might have misled lawyers, journalists and the public. In such a case, a p-value is the probability of what you see (more precisely, of at least what you see), assuming pure chance. That is not the same as the probability that pure chance was the cause of what you see – the fallacy of the transposed conditional, also known as “the prosecutor’s fallacy”.
Exercise to the reader: when is this fallacy not a fallacy? Hint: revise your knowledge of Bayes’ rule: posterior odds equals prior odds time likelihood ratio.
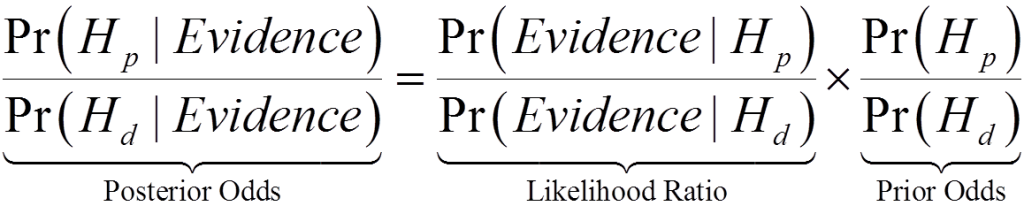
Bayes rule in odds form. p and d stand for “prosecution” and “defence” respectively, H stands for “Hypothesis”
Confounding factors
We asked the authors for the original Excel spreadsheets and for the “R” scripts they had used to process the data. They declined to give them to us, saying this would not be proper since they were confidential. We asked Daniela’s lawyer to ask the court to ask for those computer files on our behalf. The court declined to satisfy our request. We were finally sent just the Excel files by the hospital administration, a week before we were called to give evidence. Fortunately, with a combination of OCR and a lot of painstaking handwork, a wealthy friend of Daniela’s lawyer had already managed to help us get the data files reconstructed. We performed a lot of analyses with the help of a succession of students because extracting what we needed from those spreadsheets was an extraordinarily challenging issue. One kept finding anomalies that had to be fixed in one way or another. Even when we had “clean” spreadsheets, it still was a mess.
Next, we started looking for confounding factors that might explain the difference between Daniela and her colleagues, which certainly was striking and real. But was it perhaps entirely innocent?
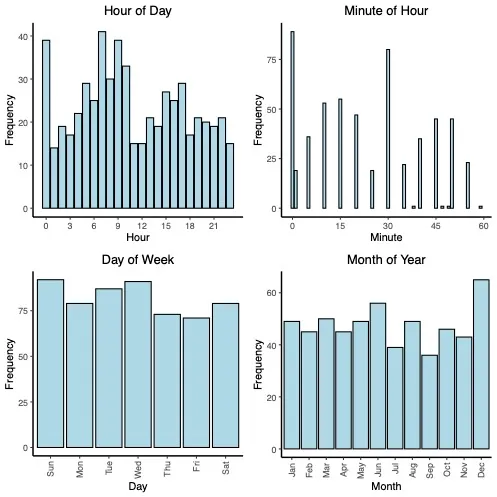
First of all, simple histograms showed that death rates on that ward varied strongly by month, with big peaks in June and again in December. (January is not high: elderly people stay home in January and keep themselves warm and safe). That is what one should expect. The humid heat and air pollution in the summer; or the damp and cold and the air pollution in the winter, exacerbated by winter flu epidemics. Perhaps Daniela worked more at bad times than at good times? No. It was clear that sectors A+B were different from C+D. Death rates were different, but also the number of beds in each wing was different. Perhaps Daniela was allocated more often to “the more difficult” sections? It was not so clear. The authors computed death rates for the whole ward, or for each wing of the ward, but never took account of the number of patients in each wing nor of the severity of their illnesses.
When deaths get processed
Most interesting of all was what we found when we looked at the hour of the time of death of patients who died, and the minute of the time of death of patients who died. Patients tended to die at times which were whole hours, “half past” was also quite popular. There was however also a huge peak of deaths between midnight and five minutes past midnight! There were fewer deaths in a couple of hours soon after lunchtime. There were large peaks of deaths around the time of handover between shifts: 7:00 in the morning, 2:00 in the afternoon, 9:00 in the evening. The death rate is higher in the morning than in the afternoon, and higher in the afternoon than at night. When you’re dying (but not in intensive care, when it is very difficult to die at all) you do not die in your sleep at night. You die in the early morning as your vital organs start waking up for the day. Now, also not surprisingly, the number of nurses on a ward is largest in the morning when there is a huge amount of work to do; it’s much less in the afternoon and evening, and it’s even less at night. This means that a full-time nurse typically spends more time in the hospital during morning shifts than during afternoon shifts, and more time during afternoon shifts than during night shifts. The death rate shows the same pattern. Therefore, for every typical full-time nurse, the death rate while they are at work tends to be higher than when they are not at work!
Nurses aren’t authorized to officially register times of death. Only a doctor is authorized to do that. He or she is supposed to write down the time at which they have determined the patient is no longer alive. It seems that they often round that time to whole or half hours. The peak just after midnight is hard to explain. The date of death has enormous financial and legal consequences. The peak suggests that those deaths may have occurred anywhere in a huge time window. Whether or not doctors come to the wards on the dot at midnight and fill in forms for any patients who have died in the few hours before is hard to believe.
What is now clear is that it is mainly around the hand-over between shifts that deaths get “processed”. Quite a few times of death are so hard to know that they are shunted to five minutes past midnight; many others are located in the hand-over period but might well have occurred earlier.
Longer shifts
Some nurses tend to work longer shifts than others. Some conscientiously clock in as early as they are allowed, before their shift starts, and clock out as late as they can after their shift ends. Daniela was such a nurse. Her shifts were indeed statistically significantly longer than those of any of her colleagues. She very often stayed on duty several hours after the official end of the official ten-minute overlap between shifts. There was often a lot to do – one can imagine often involving taking care of the recently deceased. Not the nicest part of the job. Daniela was well known to be a rather conscientious and very hard worker, with a fiery temper, known to play pranks on colleagues or to loudly disagree with doctors for whom she had a healthy disrespect.
Incidentally, the rate of admissions to Umberto I hospital tumbled down after the news broke of a serial killer – and the news broke the day after the last day the serial killer was at work, together with the publication of the lurid “selfie”. The rate of deaths was slowly increasing over the two years up to then, as was in fact also the rate of admissions and the occupancy of the ward. A hospital getting slowly more stressed? Taking on more work?
If one finds a correlation between X and Y, it is a sound principle to suppose that it has a causal explanation. Maybe X causes Y, maybe Y causes X, … and maybe W causes both X and Y, or maybe X and Y both cause Z and there has been a selection on the basis of Z. In the case of Lucia de B., her association between inexplicable incidents and her presence on the ward was caused by her, since the definition of “unexpected and inexplicable incident” included her being there. She was already known to be a weird person, and it was already clear that there were more deaths than usual on her ward. The actual reason for that was a change of hospital policy, moving patients faster from intensive care to medium care so that they could die at home, rather than in the hospital. If she was not present, then the medical experts always could come up with an explanation for why that death, though perhaps a bit surprising at that moment, was expected to occur soon anyway. But if Lucia was there then they were inclined to believe in foul play because after all there were so many incidents in her shifts.
Julia and I are certain that the difference between Daniela’s death rates and those of other nurses is to a huge extent explainable by the anomalies in the data which we had discovered and by her long working hours.
Some residual difference could be due to the fact that a conscientious nurse actually notices when patients have died, while a lazy nurse keeps a low profile and leaves it to her colleagues to notice, at hand-over. We have been busy fitting sophisticated regression models to the data but this work will be reported in a specialist journal. It does not tell us more than what I have already said. Daniela is different from the other nurses. All the nurses are different. She is extreme in a number of ways: most hours worked, longest shifts worked. We have no idea how the hospital allocated nurses to sectors and patients to sectors. We probably won’t get to know the answer to that, ever. The medical world does not put out its dirty washing for everyone to see.
Conviction, acquittal, cassation
We wrote a report and gave evidence in person in Ravenna in early 2015. I did not have time to see the wonderful Byzantine mosaics though I was treated to some wonderful meals. I think my department paid for my air ticket. Julia and I worked “pro deo“. In our opinion, we totally shredded the statistical work of the authors. The court however did not agree. “The statistical experts for the defence only offered a theoretical discourse while those of the prosecution had scientifically established hard facts”. In retrospect, we should have used stronger language in our report. The authors stated that they had definitively proven that Daniela’s presence caused 90 or so extra deaths. They stated that this number could definitely not be explained as a chance fluctuation. They stated that, of course, the statistics did not prove that she had deliberately murdered those patients. We, on the other hand, had used careful scientific language. One begins to understand how it is that experts like the authors are in such high demand by public prosecutors.
There was also toxicological evidence concerning one of the patients and involving K+ Cl–, but we were not involved in that. There was also the “selfie”, there was character evidence. There were allegations of thefts of patients’ personal jewellery. It all added up. Daniela was convicted of just one murder. The statistical evidence provided her motive: she just loved killing people, especially people she didn’t like. No doubt, a forensic psychologist also explained how her personality fitted so well to the actions she was alleged to have done.
Rapidly, the public prosecution started another case based largely on the same or similar evidence but now concerning another patient, with whom Daniela had had a shouting match, five years earlier. In fact, this activity was probably triggered by families of other patients starting civil cases against the hospital. It would also clearly be in the interest of the hospital authorities to get new criminal proceedings against Daniela started. However, Daniela’s lawyers appealed against her first conviction. It was successfully overturned. But then the court of cassation overturned the acquittal. Meantime, the second case led to a conviction, then acquittal on appeal, then cassation. All this time Daniela was in jail. Cassations of cassations meant that Daniela had to be tried again, by yet another appeal court, for the two alleged murders. Julia and I and her young colleague Francesco Dotto got to work again, improving our arguments and our graphics and our formulations of our findings.
At some point, triggered by some discussions with the defence experts on toxicology and pathology, Julia took a glance at one of the authors quite separate report on the toxicological evidence. This led to a breakthrough, as I will now explain.
No potassium chloride poisoning
The author knew the post-mortem “vitreous humour” potassium concentration of the last patient, a woman who had died on Daniela’s last day. That death had somehow surprised the hospital doctors, or rather, as it later transpired, it didn’t surprise them at all: they had already for three months been looking at the death rates while Daniela was on duty and essentially building up a dossier against her, just waiting for a suitable “last straw”! Moreover, they already had their minds on K+ Cl-, since some had gone missing and then turned up in the wrong place. Finally, Daniela had complained to her colleagues about the really irritating behaviour of that last patient, 73-year-old Rosa Calderoni.
“Vitreous humour” is the transparent, colourless, gelatinous mass that fills your eyeballs. While you are alive, it has a relatively low concentration of potassium. After death, cell walls break down, and potassium concentration throughout the body equalises. The author had published papers in which he studied the hourly rate of increase in the concentration, using measurements on the bodies of persons who had died at a known time of causes unrelated to potassium chloride poisoning. He even had some fresh corpses on which he could make repeated measurements. His motivation was to use this concentration as a tool to determine the PMI (post-mortem interval) in cases when we have a body and a post-mortem examination but no time of death. In one paper he did a regression analysis, plotting a straight line through a cloud of points (y = concentration, x = time since death). He had about 60 observations, mostly men, mostly rather young. In a second paper he fitted a parabola and moreover noted that there was an effect of age and of sex. The authors also observed the huge variation around that fitted straight line and concluded that the method was not reliable enough for use in determining the PMI. But this did not deter the author, when writing his toxicological report on Rosa Calderoni! He knew the potassium concentration at the time of post-mortem, he knew exactly when she died, he had a number for the natural increase per hour after death from his first, linear, regression model. With this, he calculated the concentration at death. Lo and behold: it was a concentration which would have been fatal. He had proved that she had died of potassium chloride poisoning.
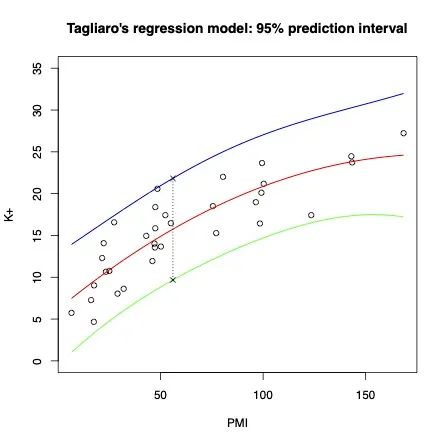
Julia and Francesco used the model of the second paper and found out that if you would assume a normal concentration at the time of death, and take account of the variability of the measurements and of the uncertainty in the value of the slope, then the concentration observed at the time of post-mortem was maybe above average, but not surprisingly large at all.
Daniela Poggiali became a free woman. I wish her a big compensation and a long and happy life. She’s quite a character.
Health care serial killers
Aside from the “couleur locale” of an Italian case, this case had incredibly much similarity with the case of Lucia de Berk. It has many similarities with quite a few other contested serial killer nurse cases, in various countries. According to a NetFlix series, in which a whole episode is devoted to Daniela, these horrific cases occur all the time. They are studied by criminologists and forensic psychologists, who have compiled a list of “red flags” intended to help warn hospital authorities. The scientific term here is “health care serial killer”, or HCSK. One of the HCSK red flags is that you have psychiatric problems. Another is that your colleagues think you are really weird. Especially when your colleagues call you an angel of death, that’s a major red flag. The list goes on.
These lists are developed in scientific publications in important mainstream journals, and the results are presented in textbooks used in university criminology teaching programs. Of course, you can only scientifically study convicted HCSKs. Your sources of data are newspaper reports, judges’ summings up, the prosecution’s final summary of the case. It is clear that these red flags are the things that convince judges and jurors to deliver a guilty verdict. These are the features that will first make you a suspect, which police investigators will look for, and which will convince the court and the public of your guilt.
Amusingly, one of the side effects of the case of Lucia de Berk was contributing a number of entries to this list, for instance, the Stephen King horror murder novels she had at home which were even alleged to have been stolen from the library. Her conviction for the theft of several items still stands. As does Daniela’s: this means that Daniela is not eligible for compensation. In neither case was there any real proof of thefts.
Amusingly, one of the side effects of the case of Lucia de Berk was contributing a number of entries to this list. Embarrassingly, her case had to be removed from the collections of known cases after 2011, and the criminologists and forensic psychologists also now mention that statistical evidence of many deaths during the shifts of a nurse is not actually a very good red flag. They have learnt something, too.
Modern-day witches
Interesting is also the incidence of these cases: less than 1 in a million nurses killing multiple patients per year, according to these researchers. These are researchers who have the phenomenon of HCSKs as their life work, giving them opportunities to write lurid books on serial murder, appear in TV panels and TV documentaries explaining the terrible psychology of these modern-day witches, and to take the stand as prosecution witnesses.
Now, that “base rate” is actually rather important, even if only known very roughly. It means that such crimes are very, very unusual. In the Netherlands, one might expect a handful of cases per century; maybe on average 100 deaths in a century. There are actually only about 100 murders altogether in the Netherlands per year. On the other hand, more than 1000 deaths every year are due to medical errors. That means that evidence against a nurse suspected of being a HCSK would be very strong indeed before it should convince a rational person that they have a new HCSK on their hands. Lawyers, judges, journalists and the public are unfortunately perhaps not rational persons. They are certainly not good with probability, and not good with Bayes’ rule. (It is not allowed to be used in a UK criminal court, because judges have ruled that jurors cannot possibly understand it).
I am still working on one UK case, Ben Geen. I believe it is yet another example of a typical innocent HCSK scare in a failing hospital leading to a typical unsafe conviction based largely on the usual red flags and a bit of bad luck. At least, I see no reason whatsoever to suppose that Ben Geen was guilty of the crimes for which he is sitting out a life sentence. Meanwhile, a new case is starting up in the UK: Lucy (!) Letby. I sincerely hope not to be involved with that one.
Time for a new generation of nosy statisticians to do some hard work.
References
Norman Fenton, Richard D. Gill, David Lagnado, and Martin Neil. Statistical issues in serial killer nurse cases. https://arxiv.org/abs/2106.00758.
Alexander R.W. Forrest. Nurses who systematically harm their patients. Medical Law International, 1(4): 411–421, 1995. https://doi.org/10.1177/096853329500100404
Richard D. Gill, Piet Groeneboom, and Peter de Jong. Elementary statistics on trial—the case of Lucia de Berk. CHANCE, 31(4):9–15, 2018. https://doi.org/10.1080/09332480.2018.1549809
Covadonga Palacio, Rossella Gottardo, Vito Cirielli, Giacomo Musile, Yvane Agard, Federica Bortolotti, and Franco Tagliaro. Simultaneous analysis of potassium and ammonium ions in the vitreous humour by capillary electrophoresis and their integrated use to infer the post mortem interval (PMI). Medicine, Science and the Law, 61(1 suppl):96–104, 2021. https://journals.sagepub.com/doi/abs/10.1177/0025802420934239
Nicola Pigaiani, Anna Bertaso, Elio Franco De Palo,Federica Bortolotti, and Franco Tagliaro. Vitreous humor endogenous compounds analysis for post-mortem forensic investigation. Forensic science international, 310:110235, 2020. https://doi.org/10.1016/j.forsciint.2020.110235
Elizabeth Yardley and David Wilson. In search of the ‘angels of death’: Conceptualising the contemporary nurse healthcare serial killer. Journal of Investigative Psychology and Offender Profiling, 13(1):39–55, 2016. https://onlinelibrary.wiley.com/doi/abs/10. 1002/jip.1434
Francesco Dotto, Richard D. Gill, and Julia Mortera. Statistical Analyses in the case of an Italian nurse accused of murdering patients. Submitted to Law, Probability, Risk (Oxford University Press). arXiv.org: TBA, 2022.












Add comment